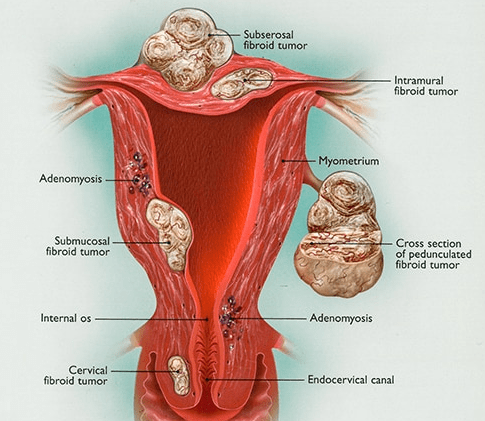
Fibroids are non-cancerous growths that develop in the uterus. A fibroid is made up from muscle fibers and fibrous tissue and is also called Myoma or Leiomyoma. They are usually asymptomatic (i.e. cause no symptoms) and appear in women of reproductive age. It is the most common gynaecological non-cancerous tumor, approximately 20-50% of women will have myomata in their lifetime.
What symptoms can they cause?
Fibroids are usually asymptomatic but they can cause: Heavy menses / Abdominal pain/ Frequent urination / Constipation / Dyspareunia (pain on intercourse) / Fertility problems.
Why do fibroids occur?
While it is not clearly known what causes fibroids, it is believed that each tumor develops from an aberrant muscle cell in the uterus, which multiplies rapidly under the influence of estrogens. There is definitely a genetic component to it, since it is more common in certain racial groups like African Americans and in close relatives.
 The name is derived from the words “Hystero”, which in Greek means uterus and the word “scope” which in Greek means to look. So hysteroscopy is a procedure where you view the internal cavity of the uterus (the endometrium) and the cervical canal.
The name is derived from the words “Hystero”, which in Greek means uterus and the word “scope” which in Greek means to look. So hysteroscopy is a procedure where you view the internal cavity of the uterus (the endometrium) and the cervical canal.
Hysteroscopy can be used for diagnostic purposes to confirm an intrauterine or cervical pathology or in order to treat certain conditions (operative hysteroscopy).
How is Hysteroscopy performed?
Diagnostic hysteroscopy can be performed in the office without anesthesia, especially if a flexible hysteroscope is available.
Operative hysteroscopy is performed under anesthesia, which is usually done in a hospital setting. The cervix is dilated to the appropriate diameter in order to accommodate the hysteroscope. The hysteroscope is a specialized telescopic camera that has 2 small canals. One canal is used to dilate the coaptating endometrial cavity with fluid (normal saline) in order to view the endometrium and the other canal is used in order to pass miniscule instruments. In more complicated hysteroscopic procedures electrosurgical instruments can be used. The procedures usually last a 10-30 minutes.
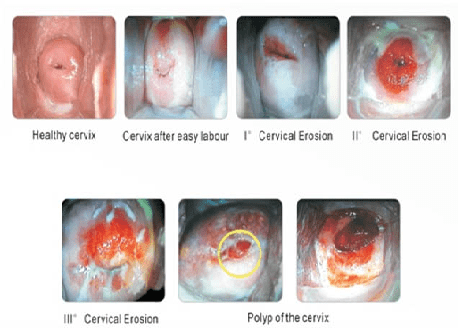
Colposcopy: A way of looking at the cervix and the vagina trough a special magnifying device called colposcope. Special stains are used to highlight any abnormal areas. If a suspicious area is identified then a small sample of tissue (biopsy) may be removed in order to confirm the diagnosis and quantify the extent of the problem. Then you can plan the appropriate therapy if needed. Colposcopy is done usually after an abnormal pap test in order to identify a lesion of HPV infection or cervicitis or a polyp.
Biopsy: A biopsy is the removal of a small amount of tissue for examination under a microscope. Other tests can suggest that cancer is present, but only a biopsy can make a definite diagnosis. A pathologist then analyzes the sample(s).
What does the HPV cause?
- Genital warts: or else condylomata accuminata are external skin growths of whitish discoloration in the genital region that can be single or accumulate in “cauliflower” like structures.
- Cervical dysplasia: is an atypical appearance of the cells lining the cervix and if it progresses it can lead to cervical cancer in several years.
How can I prevent HPV infection?
HPV is transmitted by sexual intercourse or skin to skin contact of the genital areas. Condom use decreases significantly the chances of transmission. The HPV vaccine gives immunity towards most of the HPV infections and is recommended for administration by most countries before commencing sexual intercourse. It has been shown that women with multiple sexual partners have higher chance of getting an HPV infection.
How much protection does the HPV vaccine offer?
The HPV vaccine offers more than 70% protection for cervical cancer and even greater protection for genital warts.
Is the HPV vaccine safe?
The vaccine is safe and efficient. It has been on the market for more than 10 years and several studies have looked at the side effects proving its safety. The only side affects you can get are, as in most vaccinations, local irritation, pain, fever or rarely an allergic reaction.
How can I be tested for HPV?
Genital warts: can be diagnosed by self-examination if you notice unusual growths or by your gynecologist in the annual exam by inspecting the area.
Cervical dysplasia: is diagnosed with screening tests like the Papanikolaou (Pap) smear on your annual Gyn exam. The frequency of examination depends on your age.
Does HPV cause cancer?
Yes, but luckily very few people from those exposed to HPV will eventually get Cancer.
Low grade atypia in young healthy population reverts to normal on its own in most of the cases (more than 70%).
Can I prevent cervical cancer?
Having had the vaccine and having cervical cancer screening with Pap test can prevent almost all cases of cervical cancer. This way we can identify precancerous lesions, years or even a decade before the actual cancer occurs.
How can I treat HPV infections?
Genital warts: they are usually treated with excision of the lesion and occasionally local destruction with creams/ointments, thermoablation (laser or electrocautery) or cryoablation.
Cervical dysplasias: the depth of the lesion is determined with colposcopic biopsies and then the appropriate therapy is suggested. Which could range from observation or ablation in mild cases and excision of the external portion of the cervix (cone biopsy, LEEP).
Diagnosis:
- Laparoscopy: Laparoscopy is considered the primary diagnostic modality for endometriosis. This is an invasive procedure with an overall sensitivity of 97% but with a specificity of only 77%.
- Ultrasonography – Endometriosis can be assessed by either transvaginal ultrasonography or endorectal ultrasonography.
- Magnetic resonance imaging (MRI)
Complications:
Complications of endometriosis include internal scarring, adhesions, pelvic cysts, chocolate cysts of ovaries, ruptured cysts, and bowel and ureter obstruction resulting from pelvic adhesions, endometriosis-associated infertility can be related to scar formation and anatomical distortions due to the endometriosis. Ovarian endometriosis may complicate pregnancy by decidualization, abscess and/or rupture.
Treatment:
While there is no cure for endometriosis, there are two types of interventions; treatment of pain and treatment of endometriosis-associated infertility. Non-steroidal anti-inflammatory medications, like ibuprofen, may help with the pain associated with endometriosis. Some doctors may prescribe medications that affect a woman’s hormones in order to help with endometriosis pain. Some examples are oral contraceptive pills and gonadotropin releasing hormone (GnRH) agonists, the latter of which put women into a “temporary” menopause-like state. Surgery has been shown to improve pain symptoms associated with endometriosis and may also help women become pregnant.

